

Gastroesophageal Reflux Disease (GERD)
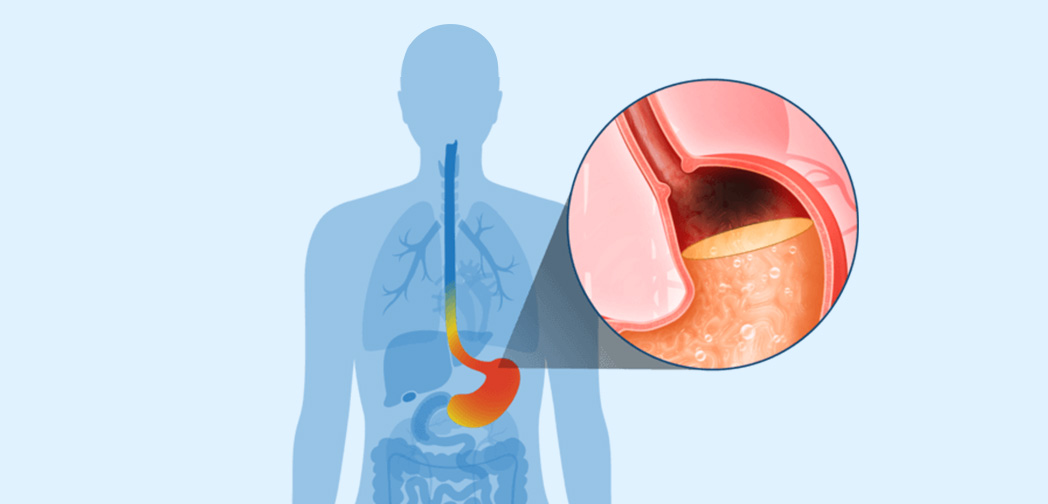
GERD results from the effects of acid on compromised mucosal defenses in the gastrointestinal tract. The reflux of gastric acid into the esophagus produces frequent and/or severe heartburn, indigestion, and reflux symptoms. Chronic GERD may damage esophageal tissue and progress to more severe diseases. GERD is one of the most prevalent diseases of any kind and is the most prevalent GI disease, affecting approximately 20% of the U.S. population and approximately 15% of the European population.
Approximately 15% to 45% of GERD patients are inadequately treated with PPIs, experiencing persistent, troublesome symptoms, such as heartburn and regurgitation.
Erosive GERD (Erosive Esophagitis) is a condition characterized by the presence of breaks, or erosions, in the esophageal tissue caused by constant irritation of the mucosal surface and subsequent loss of defense mechanisms against acid and digestive enzymes. Chronic Erosive Esophagitis can lead to complications including peptic stricture, a narrowing of the esophagus that causes difficulty swallowing, and Barrett’s esophagus, a condition in which esophageal tissue changes can progress to cancer.
In approximately two-thirds of symptomatic GERD patients, reflux symptoms are not adequately controlled after the first dose of a PPI, and nearly 50% of patients still suffer from symptoms three days later.
Non-Erosive GERD (NERD), a subcategory of GERD, is a heterogeneous disorder characterized by troublesome reflux-related symptoms in the absence of endoscopic evidence of esophageal mucosal erosions or breaks. Approximately 50-85% of patients with reflux-related symptoms that are accompanied by negative endoscopic findings are diagnosed with Non-Erosive GERD. It is estimated that more than two-thirds of GERD patients have Non-Erosive GERD.
Approximately 50-85% of patients with reflux-related symptoms that are accompanied by negative endoscopic findings are diagnosed with Non-Erosive GERD.
Available treatment for Non-Erosive GERD mainly relies on acid-suppression therapies such as antacids, histamine-2 receptor antagonists (H2RAs), and proton pump inhibitors (PPIs). PPIs are currently the most recommended therapy used in Non-Erosive GERD although these patients are typically 20–30% less responsive to PPI therapy than patients with Erosive GERD.
Non-Erosive GERD significantly impacts quality of life and is increasingly recognized as the most common cause of reflux-related symptoms in community-based populations. We believe there is a substantial need for more optimal treatments for patients.